
A Case of Postoperative Hematoma Mimicking Giant Hydrocele
Abstract
Background
In adult males, non-communicating hydroceles are non fluctuant scrotal swellings that are formed when there is an imbalance of fluid secretion and absorption between the parietal and visceral layers of the tunica vaginalis. Giant hydroceles are a rare manifestation and have previously been classified as hydroceles that drain more than 1000 mL of fluid. In this report, we describe a case of a giant hydrocele requiring surgical management and highlight a review of the literature.
Case Presentation
A 34-year-old male presented with complaints of large right-sided scrotal swelling, accompanied by scrotal discomfort. Ultrasound of the right testicle revealed a large hypoechoic space with a complex collection and posterior displacement of the testicle, indicating a possible hydrocele. The patient was taken to the operating room for a right hydrocelectomy. Approximately 2 liters of fluid were drained from the sac.
Discussion
Hydroceles are defined as straw-colored fluid collections within the parietal and visceral layers of the tunica vaginalis. Giant hydroceles, defined as fluid collections within the tunica vaginalis exceeding 1000 mL, are rare and the management of such cases is sparsely documented in the literature. While most asymptomatic fluid collections resolve spontaneously, larger collections with inflammatory changes within the testicular wall may require surgical intervention, either laparoscopic or open.
Author Contributions
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2025 Maham Qamer, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Background
In adult males, non-communicating hydroceles are non fluctuant scrotal swellings that are formed when there is an imbalance of fluid secretion and absorption between the parietal and visceral layers of the tunica vaginalis. Giant hydroceles are a rare manifestation and have previously been classified as hydroceles that drain more than 1000 mL of fluid 1, 2. Typically, hydroceles either spontaneously when the fluid imbalance corrects itself or are managed surgically through a hydrocelectomy or needle aspiration. However, giant hydroceles must be drained surgically due to the large collection of fluid and the discomfort they cause patients. In this report, we describe a case of a giant hydrocele requiring surgical management and highlight a review of the literature.
Case Presentation
A 34-year-old male presented to the Emergency Department with complaints of large right-sided scrotal swelling, accompanied by scrotal discomfort. The patient’s past medical history was remarkable for a right-sided inguinal hernia, which had been present for several years and was repaired via right open herniorrhaphy with mesh placement three months prior. Physical examination prior to the herniorrhaphy revealed a large inguinoscrotal swelling, measuring 5 inches by 6 inches. During the herniorrhaphy, a very large hernia sac was encountered that could not be fully dissected from the cord structures and required placement of two large meshes; however, the testicles were successfully reduced back into the scrotum. Ultrasound of the right testicle revealed a large hypoechoic space with a complex collection and posterior displacement of the testicle, indicating a possible hydrocele (Figure 1, Figure 2, Figure 3, Figure 4). The patient was taken to the operating room for a right hydrocelectomy. During the procedure, it was noted that the penis was buried within the scrotal swelling, necessitating the placement of a Foley catheter to identify surrounding structures. Upon incision through the Dartos fascia, significant fibrotic tissue and fluid were encountered, making it difficult to maneuver around the hydrocele sac. Upon incising the hydrocele sac, a large collection of thick, dark brown fluid resembling old blood clots was immediately aspirated. Approximately 2 liters of fluid were drained from the sac. After identifying the testicle and cord structures, the proper placement of the testicle within the scrotum was verified. Due to excessive scrotal skin, a scrotoplasty was performed prior to suturing the scrotal skin and fascia (Figure 5). The postoperative hospital course was unremarkable. The patient was discharged with plans to return to the clinic for follow-up with the surgeon.
Figure 1.Ultrasound imaging of right and left testicles in the transverse plane.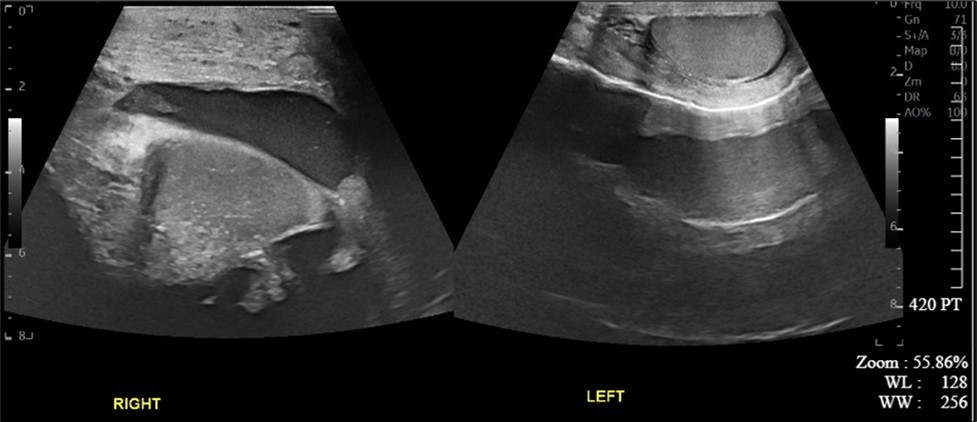
Figure 2.Ultrasound imaging in the transverse plane of the right testicle.
Figure 3.Ultrasound imaging in the transverse plane of the right inguinal region and underlying soft tissue.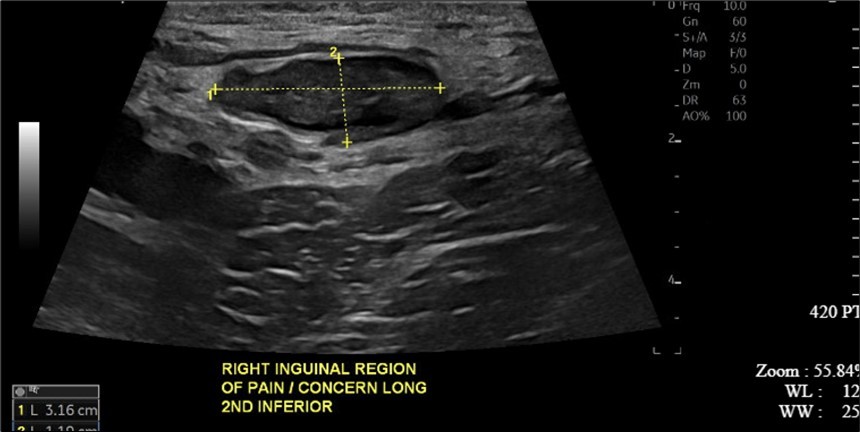
Figure 4.CT scan with contrast of the thigh region in the coronal plane with testicular swelling noted in between the thighs.
Figure 5.Testicular area status post hydrocelectomy and scrotoplasty with Penrose drain and Foley catheter in place.
Discussion
Painless scrotal swellings can be associated with various differential diagnoses, including seromas, hematomas, and hydroceles. Hydroceles are defined as straw-colored fluid collections within the parietal and visceral layers of the tunica vaginalis. Significant risk factors for hydroceles include prior inguinal herniorrhaphy, lymphatic filariasis, trauma, and a patent processus vaginalis 3. Conversely, seromas and hematomas are typically found outside of the tunica vaginalis, just beyond the scrotal skin. Postoperative fluid collections, particularly seromas or hematomas, are a common side effect of inguinal herniorrhaphy, with an overall incidence of clinical seroma formation reported as high as 60.3% during the first postoperative week and 13.2% after one month 4. Three months prior, our patient underwent an open inguinal herniorrhaphy with successful descent of the testicles back into the scrotum. However, the size of the defect created a large potential dead space, likely precipitating the collection of the large volume of fluid. The size of the dead space and fluid collection presented a diagnostic challenge that could only be confirmed after excision into the scrotum, revealing a fluid collection directly after excision into scrotal skin, and another after excision into the tunica vaginalis, raising concerns for a simultaneous hematoma and hydrocele. Since hydroceles, hematomas, and seromas are often not painful, patients may not present for surgical correction until the discomfort becomes intolerable or anxiety about hernia recurrence arises, further complicating diagnoses due to accumulation of inflammatory and fibrotic tissue.
According to the classification system suggested by Morales-Conde et al., seromas can be classified into five types: Type 0, indicating no seroma; Types I and II, representing clinical seromas lasting between one to six months but requiring no treatment; Type III, symptomatic seromas manageable medically; and Type IV, seromas necessitating surgical treatment. The former two are classified as incidental seromas, while the latter two are considered complications 5. Our patient’s collection required surgical correction, falling under Type IV and being classified as a complication. It has been suggested that complete dissection of the cord structures from the hernia sac limits seroma formation. However, in our case, the original hernia defect was extremely large, rendering complete dissection difficult and resulting in incomplete dissection of the hernia sac 6.
As giant fluid collections are relatively rare, the management of such cases is sparsely documented in the literature. Ungureanu et al. described a case of scrotal swelling post-laparoscopic unilateral total extraperitoneal procedure measuring 12 cm by 14 cm 7. Ultrasound examination revealed a fluid collection despite postoperative drain placement. The collection was aspirated using an open approach, yielding 300 mL of seroma fluid. This case underscores the importance of thorough management of the hernia sac to limit seroma formation postoperatively. Further reports by Chihan et al. suggest that 90% of asymptomatic postoperative seromas will spontaneously resolve within one month 8.
Conclusion
Giant hydroceles, defined as fluid collections within the tunica vaginalis exceeding 1000 mL, are rare and often challenging to manage. The scarcity of such cases in the literature limits our understanding of their risk factors and optimal management strategies. While most asymptomatic fluid collections resolve spontaneously, larger collections with inflammatory changes within the testicular wall may require surgical intervention, either laparoscopic or open. This case underscores the importance of meticulous management of the hernia sac during inguinal herniorrhaphy to prevent the formation of extensive postoperative fluid collections. Addressing potential dead spaces at the time of repair is critical to reducing patient discomfort, anxiety, and the need for subsequent surgical interventions. Further contributions to the literature are essential to improve prevention, diagnosis, and treatment of this uncommon complication.
Acknowledgements
None.
References
- 1.Hirano S, Kawaguchi S, Mikawa I, Motoi I, Masuda S. (1991) [Giant hydrocele: two case reports]. Hinyokika kiyo. Acta Urologica Japonica. 37(2), 195-198.
- 3.Latabi A, Lakmichi M A, Dahami Z, Moudouni M S, Sarf I. (2018) Giant abdomino scrotal hydrocele: a case report with literature review. Pan Afr Med J. 28, 213-10.
- 4.JKM Fan, Liu J, Chen K, Yang X, Xu X et al. (2018) Preperitoneal closed-system suction drainage after totally extraperitoneal hernioplasty in the prevention of early seroma formation: a prospective double-blind randomised controlled trial. Hernia. 22(3), 455-465.
- 5.Morales-Conde S. (2012) A new classification for seroma after laparoscopic ventral hernia repair. Hernia. 16(3), 261-7.
- 6.Chowbey P K, Pithawala M, Khullar R, Sharma A, Soni V et al. (2006) Complications in groin hernia surgery and the way out. J Minim Access Surg. 2(3), 174-7.