Delayed Diagnosis of Glioblastoma due to Recent Ruptured Aneurysm. A Case Report.
Abstract
Rupture of an intracranial aneurysm may cover for a long time clinical and radiological signs of a coexistent tumor. We report the delayed diagnosis of glioblastoma in a 65-years old female with recent history of subarachnoid hemorrhage. In the literature are described few similar cases: we briefly discuss the management in the rare occurrence of a double neurosurgical disease.
Author Contributions
Academic Editor: Llumiguano Carlos, Neurosurgeon, M.D., Ph.D.Assoc. Prof. - Universidad San Francisco de Quito, EcuadorHospital Vozandes Quito, EcuadorHospital Quirón, Ciudad Real, Spain
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Gabriele Ronchetti, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Spontaneous subarachnoid hemorrhage (SAH) is a well-known and relatively common consequence of intracranial aneurysms rupture.1, 2 The clinical and radiological evolution of such a condition -including CT abnormalities lasting weeks, and possible confounding factors like vasospasm and hydrocephalus- may occasionally prevent the concurrent diagnosis of other cerebral diseases present before the hemorrhage. Here we report the case of a frontal glioblastoma late diagnosed because of the previous rupture of an anterior communicating artery aneurysm.
Case Description
A 65 years-old woman with no relevant medical history was carried to the emergency department of another institution for the sudden onset of headache and vomiting, followed by loss of consciousness. She underwent a cerebral CT scan, that showed diffuse SAH in the basal cisterns and anterior interemispheric fissure (Figure 1). The CT angiogram displayed a single aneurysm of the anterior communicating artery, that local radiologists considered unfavorable for endovascular treatment. The patient was therefore surgically managed, with left pterional craniotomy for aneurysm clipping and right external ventricular drain (EVD) positioning. In the following days the woman reacquired alertness; the EVD was removed without need of permanent shunting and she was transferred to rehabilitation four weeks after the operation in quite good conditions.
Figure 1.Non-contrast axial CT scan showing thick subarachnoid hemorrhage in the basal cisterns and in the frontal interemispheric space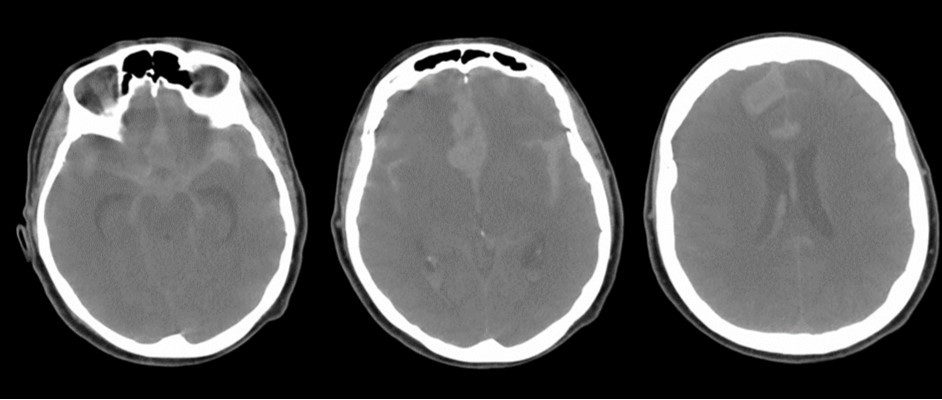
Figure 2.Follow-up at 6 weeks. The vascular clip is in place. Ventricles are quite enlarged. The region of the corpus callosum appears altered
The follow-up CT scan made two weeks later showed a mild ventricular enlargement and persistent density alterations in the frontal region (Figure 2) that were interpreted as normal. Once discharged at home, the patient developed progressive disorientation that finally let her refer to our hospital for consult four months after aneurysm clipping. The cerebral CT we performed showed further ventricular growth, and a tumor-like image in the right frontal lobe (Figure 3). She was admitted to our ward and underwent a contrast-MRI that confirmed the suspicion of aggressive intra-axial neoplasm (Figure 4). The week after, under general anesthesia we performed a right craniotomy and removed a large part of the tumor, sparing the portion going through the corpus callosum (Figure 5). During convalescence the patient had few epileptic attacks, treated with drugs. A mild cognitive impairment persisted after surgery, without focal motor deficits. The gait, limited and unstable since the SAH, remained poor and the patient never walked again after the operation. The histological examination indicated a WHO grade IV glioma: IDH1-p53 negative glioblastoma. The patient and her relatives refused a ventriculo-peritoneal shunt after knowing this unfortunate diagnosis. Transferred to rehabilitation, the woman made just a short low-dose chemotherapy cycle and finally died four months after tumor resection.
Figure 3.4 months non-contrast CT scan. Ventricles are dilated. A mass clearly affects the right frontal and midline region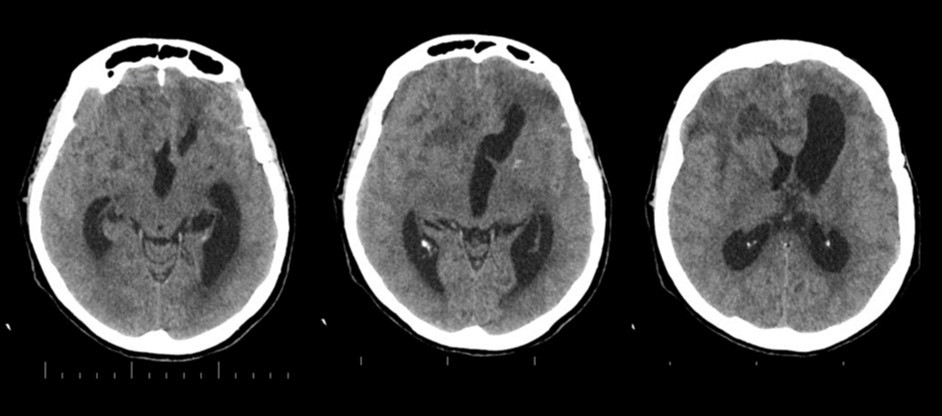
Figure 4.Pre-operative contrast axial, coronal and sagittal MRI. Glioma of the right frontal lobe, extending contralaterally
Figure 5.Post-operative non-contrast CT scan. Subtotal removal of the tumor, sparing the corpus callosum area. Partial relieve of mass effect on the ventricles, that remains enlarged
Discussion
Glioblastoma is the most malignant and -unfortunately- frequent glial tumor in adults. Symptoms and signs may vary according to size and location, and usually progress in some weeks. The clinical presentation may be occasionally acute due to hemorrhage inside of the lesion.3, 4
Aneurysmal subarachnoid hemorrhage has a sudden clinical onset, but later entails a complex syndrome including persistent CT alterations in the region of bleeding, persistent neurological impairment, and in some cases vasospasm and hydrocephalus.
The clinical and radiological features of these two diseases are perfectly known to neurosurgeons; anyhow our case shows that trouble rises when they do occur simultaneously. The patient we described had initially acute signs due to SAH and later signs that were incorrectly interpreted as SAH-related. The tumor was almost invisible -because of its likely small volume and thick SAH- in the first CT performed (Figure 1). Analyzing the early follow-up CT (Figure 2) anyway things do not seem so clear. In the frontal region remained too much fogging close to the midline; the asymmetric distribution of such alteration should had point out a problem, but everybody kept thinking to a “simple” post-hemorrhagic condition, due to ventricular enlargement and focal ischemia. The initial mental impairment of that period was equally attributed to a normal SAH result with moderate hydrocephalus. The proper diagnosis of glioma happened late, and the patient was at that point unable to have significant benefits from surgery.
High grade gliomas typically harbor vascular changes and neo-angiogenesis. Biochemical agents and local hyperemia may stress both veins and arteries within the tumor, leading to rupture and hemorrhage or thrombosis and ischemia. A real well-defined arterial aneurysm is anyhow an uncommon finding in glioblastoma patients, especially if the feeding vessel of the aneurysm is not within the tumor territory. In the literature we found just few cases described: most were unruptured aneurysm.5, 6, 7, 8, 9, 10, 11, 12, 13 We are not sure about any pathological link between the aneurysm and glioma in our patient. It is extremely likely that these two diseases developed simultaneously for a while, without interfering one each other. The most important issue in our opinion has been the diagnosis, rather than the treatment that did not result per se particularly difficult in any of the two pathologies. If the medical team -radiologists, neurologists, neurosurgeons- had acquired an increased sensibility (when evaluating the initial neurological impairment and the not-so clear radiological findings of the patient) the diagnosis of glioblastoma would arrive earlier than what actually happened, giving more chances of a longer survival.
Conclusions
This is one of the first descriptions of aneurysmal subarachnoid hemorrhage followed by a glioblastoma diagnosis.
The evaluation of both clinical and radiological aspects should be always prejudice-free to allow the early diagnosis of two different diseases in the same patient. At the onset of a (even small) suspicion of a second illness, proper analyses should be always arranged to allow early clarification.
Abbreviations
SAH = subarachnoid hemorrhage.
EVD = external ventricular drain
References
- 1.King J T Jr. (1997) Epidemiology of aneurysmal subarachnoid hemorrhage. , Neuroimaging Clin N Am 7(4), 659-68.
- 2.Ingall T, Asplund K, Mahonen M, Bonita R. (2000) A multinational comparison of subarachnoid hemorrhage epidemiology in the WHO MONICA stroke study. , Stroke 31(5), 1054-61.
- 3.Iwama T, Ohkuma A, Miwa Y, Sugimoto S, Itoh T. (1992) Brain tumors manifesting as intracranial hemorrhage. Neurologia Medico-Chirurgica;32:. 130-5.
- 4.Schrader B, Barth H, Lang E W, Buhl R, Hugo H H. (2000) Spontaneous intracranial haematomas caused by neoplasms. , Acta Neurochir (Wien) 142, 979-85.
- 5.DePaulis D, Nicosia G, Taddei G, H Di Vitantonio, Gallieni M. (2016) Intracranial aneurysms and optic glioma-an unusual combination: a case report. , J Med Case Rep 10, 78.
- 6.Chamberlain M C. (2016) Co-existence of glioblastoma and cerebral aneurysm. , CNS Oncol 5(1), 9-10.
- 7.H S Nguyen, Doan N, Gelsomino M, Shabani S, Mueller W. (2015) Coincidence of an anterior cerebral artery aneurysm and a glioblastoma: case report and review of literature. Int Med Case Rep J.;8:. 295-9.
- 8.Ali R, Pabaney A, Robin A, Marin H, Rosenblum M. (2015) Glioblastoma and intracranial aneurysms: Case report and review of literature.Surg Neurol Int.;6:. 66.
- 9.Cheng W Y, Shen C C. (2004) Minimally invasive approaches to treat simultaneous occurrence of glioblastoma multiforme and intracranial aneurysm-case report. , Minim Invasive Neurosurg 47(3), 181-5.
- 10.A De Chiara, Benvenuti D, Maiuri F, Giamundo A, Lavano A. (1986) Association of internal carotid aneurysm and temporal glioblastoma. , Neurochirurgia(Stuttg) 29(2), 58-60.
- 11.Honda M, Kamada K, a Y N, Harada T, Iwanaga H et al. (1980) The association of cerebral aneurysm with malignant brain tumor-report of a case. No Shinkei Geka. 8(11), 1065-70.